
Current literature shows that interaction with urban greenery can have a wide range of positive health outcomes. Targeted nature-based programs, such as therapeutic horticulture, have been shown to result in multiple health benefits for older adults residing in temperate environments, but much less research has been carried out on populations with different phenotypes, such as older Asian adults in the tropics. The current study investigated the effects of a 24-session therapeutic horticulture program on 47 older participants in Singapore, with an experimental pretest posttest design. We found that participants maintained healthy sleep patterns and psychological health, as well as showed reduced anxiety and improved cognitive functioning (p < 0.05). In addition, they reported an increase in mean happiness score after each session. This study provides new evidence using a comprehensive set of indicators across the affective, cognitive, functional, psychosocial and physical domains, supporting current literature on the benefits of nature programs, with a novel focus on tropical environments. It provides evidence that the nature-based intervention has the potential to be translated to programs to benefit older adults in the tropics.


Highly urbanised environments offer productivity and convenience, but they also contain more stressors that affect health negatively, such as higher heat load, carbon emmissions and pollution, compared to the rural environments 1 . The positive association between contact with urban nature and health has been well established in literature. Back in the 1860s, city planners were already pronouncing that nature both tranquilizes and enlivens the mind; reinvigorating one’s whole system 2 . The number of scientific manuscripts published on the subject has also increased exponentially in the recent years, reporting wide-ranging benefits, from lower mortality 3 and morbidity 4 to improvements in physical and mental health 5 . Findings from the meta-analyses show statistically significant associations with a wide range of health benefits, including reduced diastolic blood pressure, heart rate, salivary cortisol, incidence of type II diabetes and stroke, cardiovascular and all-cause mortality, as well as health-denoting associations with pregnancy outcomes, HRV, and HDL cholesterol, and self-reported improvements in health 6 . However, most of the research was conducted in temperate regions, offering very limited understanding on the health effects of nature exposure in regions with different climatic and environmental factors, such as the tropics 7 .
Although the benefits of nature exposure on health are well established, the specific mechanisms and pathways are still not well understood. One of the leading theories is the Biophilia Hypothesis, which proposes that love for nature and ability to thrive in a natural environment are inherent to humans, dictated by evolutionary drives and instincts 8 . In contrast, biophobia, the affiliation with technology and human artifacts, is deemed to be culturally acquired rather than inborn, and as such unnatural 9 . Consequently, the healing properties of nature exposure are thought to be due to returning to our basic instincts and natural predispositions. Another commonly cited theory is the Attention Restoration Theory (ART), which proposes that contact with nature provides humans a softly fascinating environment that allows the mind to restore attentional fatigue. Nature enables people to be engaged in an “effortless” state of mind, as compared to other physical environments, which demand directed attention and hence exhaust our cognitive resources 10 .
The benefits of contact with nature are particularly well documented for older adults 11 . One nature-based activity that is known to be popular with older adults is gardening. It has been shown to promote overall health and quality of life, physical strength, fitness and flexibility, cognitive ability, and socialization 12 . A treatment related to gardening is therapeutic horticulture (TH). This is a facilitated process through which participants enhance their well-being by being involved in plant and plant-related activities. Due to its documented benefits, TH is gaining importance and TH programs are found in a wide variety of healthcare, rehabilitative, and residential settings in North America and a few other temperate countries such as the United Kingdom and Japan. A systematic review on the effects of TH showed that there was pre-post improvement in well-being, anxiety and depression, social relations, cognitive and functional outcomes 13 . Of the 20 studies included in the review, 16 were conducted on participants from long-term residential care facilities, and as such the results cannot be generalized to communities or day-care settings 13 . Only one study was conducted in the tropical environment, where the study population was healthy older adults with good cognitive functioning and good mobility 14 . Therefore, whether TH is effective for the general older adult population residing in the tropics, and its impact on a range of physical and cognitive status measures requires further investigation. Moreover, long-term outcomes of TH on physical and mental health are largely unexplored.
The current study investigated the long-term effects of a 24 session (6-month) TH program on older adults (n = 47) from three senior day-care centers. The study aimed to provide a better understanding of TH programming in the tropical environment and its health outcomes among older adults in Singapore. The TH program aims to promote enhanced health and wellbeing. We hypothesized that participants would, over time, show improvements in perceived physical health, sleep hygiene, depression, anxiety, cognitive performance (orientation, attention, memory, language, spatial visualization and motor skill), and social connectedness. We also hypothesized that the program would improve momentary positive affect immediately after each session.
Elderly participants (n = 47, 33 females) with a mean age of 77.5 years (SD = 7.8, range 60–95) were recruited progressively from three senior day care centers (SAC) in Singapore, between May 2017 to December 2018. 12 participants were first recruited from SAC 1 and assigned to group 1. They received the intervention from May to October 2017. This was followed by group 2 (intervention from November 2017 to May 2018) which comprised another 7 participants from SAC 1, and group 3 (intervention from June to December 2018) which comprised 11 participants from SAC 2, and group 4 (intervention from January to July 2019) which comprised 9 participants from SAC 3, and lastly group 5 (intervention from January to July 2019 and carried out on days different from group 4) which comprised 8 participants from SAC 3. All participants from SAC 1 (n = 19, 14 females), SAC 2 (n = 11, 8 females) and SAC 3 (n = 17, 11 females) gave consent to participate in the Mini Mental State Exam (MMSE) 15 to test for signs of dementia. An age and education adjusted formula MMSEadj = Raw MMSE − (0.471 × [education − 12]) + (0.131 × [age − 70]) was used to adjust the MMSE scores for those older than 75 years old 16 . We used the cut-off score of 17 and lower as an exclusion criterion, as an indicator of severe cognitive impairment 17 . Those excluded were deemed to benefit from a more individualized horticultural therapy treatment program. The distribution of age and years of education was balanced in the three SACs. The study was approved by the National Healthcare Group Domain Specific Review Board (DSRB), with the reference L2016/00949. The research was performed in accordance with relevant guidelines and regulations. All participants provided informed consent.
The intervention was a 24-session weekly TH program comprising an equal mix of horticultural-based and nature art activities. The program was developed with the input of a horticultural therapy expert registered with the American Horticultural Therapy Association (AHTA). In addition, we incorporated knowledge of local plants and related activities. The one-hour sessions followed a planned order, beginning with a series of introductory horticultural-based activities—growing pea sprouts, setting up planters, growing vegetables from different modes. This was alternated with a few sessions of simple nature-art activities (e.g. making sun-catchers, leaf sketching) before another few sessions of horticultural-based activities. The program is outlined in Table 1. All the sessions are designed to stimulate engagement of participants’ senses through touching, seeing and smelling the plant materials. While nature-art activities promote a sense of creativity and achievement, offering immediate gratification, horticultural-based activities encourage a waiting and nurturing attitude, offering a deep sense of purpose in the longer term. Hence, the combination of the two types of activities enabled the participants to experience complementary benefits throughout the program. The team of 4 who facilitated the program comprised personnel with experience in conducting urban farming workshops for older adults and they have received training by the AHTA registered horticultural therapy expert.
We used the ANOVA repeated measures to compare the group means at the different time points, and Greenhouse–Geisser correction was applied where homogeneity of variance assumption was violated. Bonferroni corrected means were reported for the post-hoc comparisons. The paired-samples t-test was used to determine whether there was a statistically significant mean difference in individual VAS scores of happiness level before and after each session. All analyses were performed using IBM SPSS Statistics version 26. Alpha level of 0.05 was used as a level of statistical significance. Due to follow-up issues after the completion of the intervention, the responses at timepoints 3 (9-month) and 4 (12-month) dropped to 38 and 44 respectively. The cases with missing values were omitted in the pairwise comparisons.
The general baseline characteristics of the participants are summarized in Table 2. The majority were females above 70 years old, of Chinese ethnicity and retired. The sample varied in socio-economic status, as indicated by housing type and years of schooling. Six participants required assistance to move about during the intervention, either in the form of wheelchair or walking aids.
Table 2 Baseline characteristics of the study participants.We measured participants’ happiness level before and after each session using the VAS. 753 sets of pre-post responses from 35 participants were collected and analyzed. A score of “10” represents the happiest whilst “1” represents most unhappy. Post-session VAS scores was higher (M = 9.49, SD = 0.88) than pre-session scores (M = 8.88, SD = 1.34), a statistically significant increase of 0.60 [95% CI 0.53–0.67), t(752) = 16.32, p < 0.0005], with medium effect size (d = 0.61).
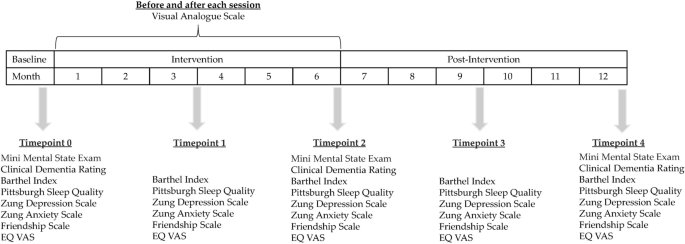
We measured outcomes in the cognitive, functional psychosocial and physical domains at the timepoints illustrated in Fig. 1. Mean values at each time point and the results of statistical analyses for all the outcomes are summarised in Table 3.
Table 3 Summary of outcomes at the different timepoints and changes in outcomes over time.The highest possible score for MMSE is 30, representing maximum cognitive performance. The results showed that there was statistically significant difference in mean MMSE score among the three time points measured. The TH treatment elicited a statistically significant increase of 0.87 in participants’ mean MMSE score at time point 2 compared to baseline, p = 0.01. At time-point 4, six months post treatment, there was a marginal drop of MMSE score by 0.07, but this was not statistically significant.
The scoring of CDR ranges between 1 and 5. A score close to 0 indicates no dementia and a score of 1 indicates mild dementia. A higher score corresponds to an increasing severity in one’s cognitive decline 32 . The CDR was administered to assess if any participants had risks of dementia during the 24-month period. We had the intention of referring them for follow-up if needed. The results showed that there was a mild but statistically significant increase in the CDR scores over time, but overall, the scores were within the healthy range of close to 0.
The maximum score of 100 represents a fully independent subject capable of performing basic ADL whereas the lowest score of 0 represents a totally dependent state 27 . The results showed that the mean scores in BI were close to 100 at all the five timepoints. There was no significant difference in the scores among the timepoints.
All 7 questions are scored on a scale of 0–3, whereby 3 reflects the negative extreme. The maximum global score for PSQI is 21. A score of 5 or greater indicates a poor sleeper 33 . The results showed that the participants maintained healthy sleep quality at all the timepoints measured. They showed marginally better PSQI global scores compared to baseline during the intervention period at timepoints 2 and 3, but this was not significant (p > 0.05).
Participants’ depression and anxiety states were assessed using SDS and SAS. The mean SDS and SAS scores at time points 0, 1, 2 3 and 4 are summarised in Table 3. They are below the cut-off points for clinical relevance of SDS 34 and SDA 35 , which are 50 and 40 respectively. Higher scores indicate presence of depressive and anxiety disorders. The results showed that participants’ SDS and SAS scores were within the healthy range at all the five timepoints. There was marginal improvements (reduction) in mean SDS scores at the different timepoints compared to baseline but this was not significant. On the other hand, there was significant improvement in SAS scores across the time points. Compared to baseline, the TH intervention elicited significant improvements in mean SAS scores at timepoints 2 and 3, by − 2.18 ± 0.90 (p < 0.05) and − 1.87 ± 0.60 (p = 0.03).
Participants’ sense of social connectedness was assessed using the FS. There was no significant difference in mean FS scores among the different timepoints, and all the scores were equivalent to being socially connected.
There were no significant differences in the mean EQ VAS scores across the different time points. The mean scores for participants aged 65–74 and 75 and above are summarised in Table 4.
Table 4 Mean EQ VAS scores in participants of two age groups during and after intervention.The current study provided evidence in support of the existing literature on the effectiveness of TH in enhancing well-being of older adults, filling the information gap for the Asian phenotype in the tropical environment and providing novel information on the long-term effectiveness. The intervention resulted in several health benefits for the participants, namely more positive momentary affect, improved cognitive function and reduced anxiety. The effects of the latter two areas were sustained for up to 6 months after the intervention was completed. Throughout and six months after the intervention, the participants sustained their functional performance, maintaining healthy BI and PSQI scores. This is deemed to be a positive outcome, considering majority of them were aged 70 years and above, and would normally deteriorate in functional health in the span of one year. Similarly, they maintained a non-depressive state and a healthy ED VAS score. The mean EQ VAS scores for participants who were aged 65–74 years (n = 15) and 75 years and above (n = 29) during and after the intervention were consistently better that the population norm in the same age group in Thailand 36 and the United Kingdom 37 . Overall, this study has demonstrated the positive effects of the 24-week TH on older adults in the tropics, in improving their momentary positive affect, cognitive performance and reduced anxiety over time.
Urban nature supports health by functioning as “salutogens”, factors in the environment that support health and well-being 38 , to promote positive experiences and behavior. Its benefits on the health and wellbeing of older adults have economic importance, considering the societal expenditures on health and related services for the group. Singapore, with 100% urban population, is expected to have more than 20% of its population over the age of 65 years by 2030. According to a recent survey "Understanding the Quality of Life of Seniors in Singapore", older adults in the country reported a lower quality of life than the general population in areas such as recreation, leisure and affect. We think that Singapore is well placed to introduce nature-based solutions to improve the quality of life of the older adult population, considering the profuse greenery and accessible green spaces managed throughout the entire island. Moreover, older adults have more hours of leisure time, and stand to derive deeper benefits by taking part in TH as a form of nature-based recreation and occupation.
There are several limitations to the study. For ethical reasons, a pretest posttest methodology was selected over a randomized control trial as the recruitment centres raised concerns about withholding the treatment from the potential control group. Additionally, budget constraints precluded adopting a waitlist randomized control trial approach. We were not able to include biological makers as objective assessments, as we had done in our past study 14 , for technical reasons linked to sample storage. The strength of this study was the long-term assessment of a lifestyle nature-based programme that measured several cognitive, executive function, lifestyle and behavioural outcomes in the often-overlooked population of older adults, with a relatively low drop-out rate.
The current study evaluated the effects of a 24-week TH intervention programme on older adults conducted in the Therapeutic Garden @HortPark (Singapore), which has been specifically designed to support mental and physical health. The therapeutic programme was centred around nature exposure and caring for plants, a nurturing process that has been shown to promote physical and mental health, as well as development of a personal relationship with nature. The TH program promoted understanding and exploration of nature and cultivated a sense of purpose in the participants. In addition, we found that the participants maintained healthy sleep, psychological health and showed improved cognitive functioning over time. This study provides evidence that structured nature-based programmes play a positive role in maintaining and enhancing the physical and mental health and wellbeing in older populations. We conclude that the 24-week TH program is a promising intervention to be extended in other SACs in Singapore, to improve the wellbeing of older adults. We recommend that TH be introduced as a part of healthy aging recommendations in tropical climates and beyond.
The data that support the findings of this study are available from the corresponding author, A.S., upon reasonable request.